
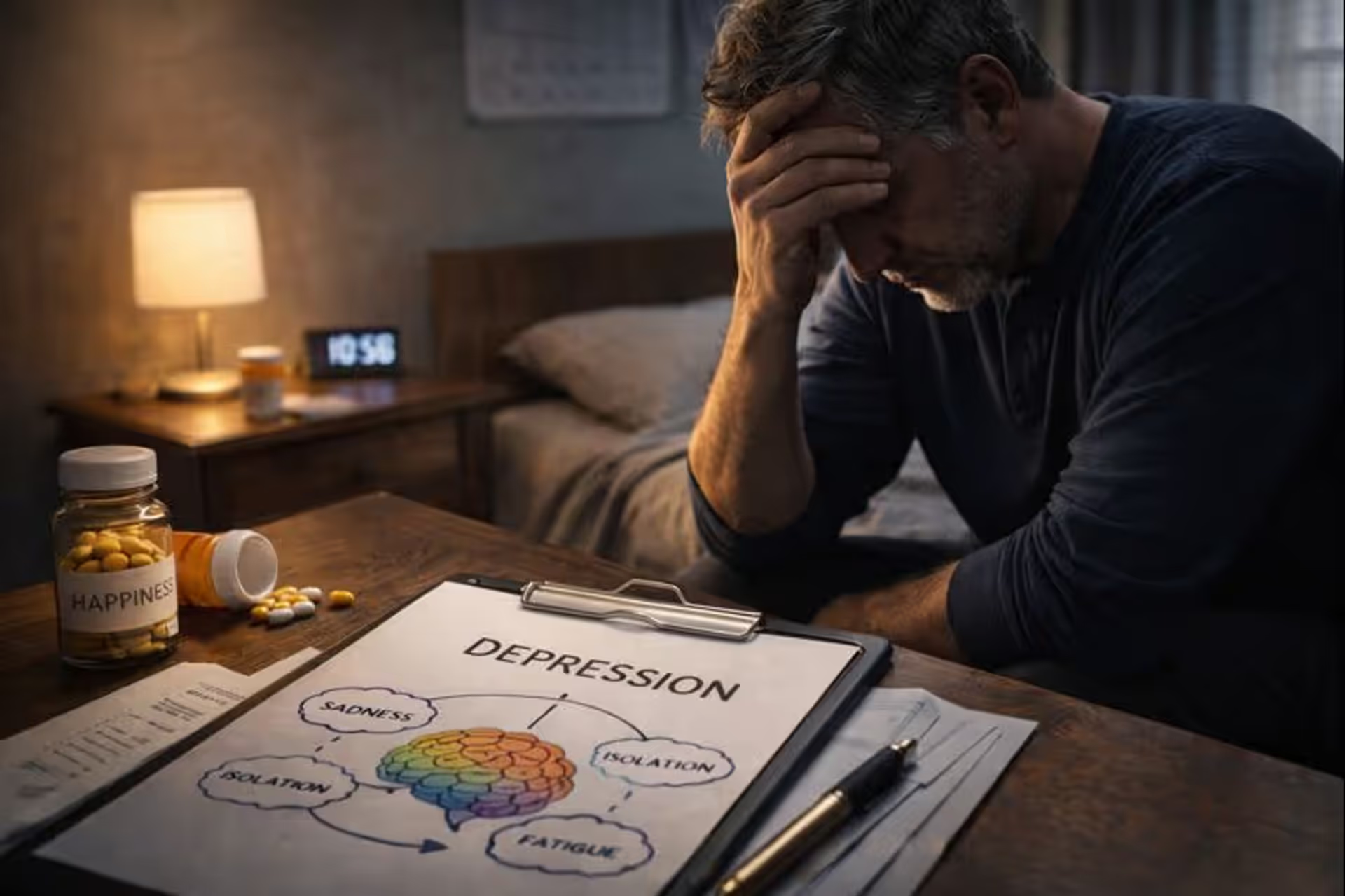
Success can mask inner suffering
High-Functioning Depression Signs Guide

Content
Content
She runs a successful business, maintains an active social life, and never misses a workout. Her Instagram shows beach vacations, dinner parties, and career achievements. By every external measure, she's thriving. Yet every morning she fights just to get out of bed. Every smile takes conscious effort. Every accomplishment feels hollow. She wonders constantly: if my life looks so good, why do I feel so empty?
This is high-functioning depression — a form of depression that hides behind competence, achievement, and carefully maintained appearances. Unlike the stereotypical image of depression (unable to work, withdrawn from life, visibly struggling), people with high-functioning depression continue performing at high levels while experiencing persistent internal suffering that few people ever see.
The term has exploded across social media, with millions recognizing themselves in descriptions of smiling depressionand walking depression. TikTok and Instagram creators sharing their experiences have sparked a collective realization: depression doesn't always look like the textbook description. Sometimes it looks like the most put-together person in the room.
High-functioning depression isn't an official clinical diagnosis but describes a very real experience — often corresponding to Persistent Depressive Disorder (dysthymia) or other depressive conditions where symptoms are chronic but not severe enough to completely disable daily functioning. The danger lies precisely in this functionality: because life continues, because work gets done, because appearances are maintained, the suffering goes unrecognized — often even by the person experiencing it.
High-functioning depression is perhaps the most dangerous form because it's so easy to dismiss. People think 'I can't be depressed — I'm successful, I'm productive, I'm handling my responsibilities.' But depression doesn't require visible dysfunction. Some of my most accomplished patients have been the most depressed, and their success became another reason to invalidate their suffering. They'd achieved everything they thought would make them happy and still felt empty.
— — Dr. Amanda Foster, Clinical Psychologist and Depression Specialist, Columbia University Medical Center
Understanding the signs of hidden depression enables earlier recognition and intervention. This guide examines the warning signs most people overlook, explains the deep psychological mechanisms behind high-functioning depression, and provides pathways toward help and healing.
Understanding the Paradox: Success and Suffering Coexisting
Why Depression and Achievement Aren't Mutually Exclusive
The popular conception of depression involves visible incapacity — someone unable to get out of bed, missing work, withdrawing completely from life. This image, while accurate for some depression presentations, creates a dangerous blind spot. It suggests that functioning equals wellness, that productivity proves mental health, that achievement and depression cannot coexist.
This misconception stems from misunderstanding what depression actually is. Depression is fundamentally a disorder of internal experience — of mood, energy, pleasure, and meaning — not necessarily of external behavior. The internal experience can be profoundly impaired while external behavior continues through willpower, habit, fear, or necessity.
Consider an analogy: chronic pain. Someone with chronic back pain might continue working, socializing, and meeting responsibilities. Their functionality doesn't mean the pain isn't real or doesn't deserve treatment. The pain exists regardless of what they manage to accomplish despite it. High-functioning depression operates similarly — the internal suffering is real regardless of external achievements.
What makes high-functioning depression particularly insidious is how achievement can become both mask and reinforcement of the condition. Success provides evidence against depression ("I can't be depressed — look at what I've accomplished"), while the emptiness following achievement reinforces depressive beliefs ("Even success doesn't make me happy — something must be fundamentally wrong with me").
The Hidden Cost of Maintaining Appearances
People with high-functioning depression often describe their daily experience as exhausting performance. Every interaction requires effort. Every task demands energy they don't have. Every smile is conscious choice rather than natural response. They're running a marathon while appearing to stroll casually.
This performance extracts enormous psychological cost. The energy spent maintaining appearances isn't available for genuine living, connection, or recovery. The gap between external presentation and internal reality creates chronic inauthenticity that compounds the depression. And the success of the performance — the fact that no one notices the struggle — reinforces isolation and the belief that no one would understand or help even if they knew.
The tragedy is that the very coping mechanisms that enable continued functioning often prevent recovery. The perfectionism that drives achievement also drives self-criticism. The emotional suppression that enables professional composure also blocks access to feelings needed for healing. The self-reliance that handles responsibilities without asking for help also prevents reaching out when help is desperately needed.

Author: Evan Miller;
Source: psychology10.click
The Psychological Architecture of High-Functioning Depression
The Achievement-Identity Fusion
Many people with high-functioning depression have constructed identities fundamentally built on achievement and competence. Their sense of worth, their understanding of who they are, depends on performance. This isn't vanity — it often develops from childhood experiences where love felt conditional on achievement, where failure meant withdrawal of approval, where being "good" meant being accomplished.
When depression emerges in someone with achievement-fused identity, acknowledging it threatens the very foundation of self. Admitting depression means admitting imperfection, which feels like admitting worthlessness. The person faces an impossible choice: acknowledge depression and lose identity, or deny depression and lose sanity. Most choose denial, at least initially.
This denial isn't conscious dishonesty — it's psychological self-preservation. The mind genuinely cannot recognize what recognizing would destroy. Symptoms get reframed: exhaustion becomes "I just need more sleep," emptiness becomes "I need a new challenge," irritability becomes "work stress." Each reframe preserves identity while allowing depression to deepen unaddressed.
The achievement-depression cycle intensifies over time. The person feels empty or inadequate, so they pursue achievement to feel worthy. Achievement produces brief satisfaction, then emptiness returns, now with added evidence that even success doesn't help. This confirms deep inadequacy beliefs, driving more frantic achievement-seeking. Each cycle depletes more energy while providing less satisfaction, until the person is exhausted, empty, and unable to understand why everything they've accomplished hasn't made them happy.
Emotional Suppression as Survival Strategy
High-functioning depression often develops in people who learned early that emotions were problems to be managed rather than experiences to be felt. Perhaps they grew up in families where emotional expression was discouraged, where they needed to be the "strong one," where showing vulnerability meant being criticized or abandoned.
These individuals developed exceptional emotional management skills — the ability to suppress feelings, maintain composure under pressure, continue functioning regardless of internal state. These skills serve them well professionally and socially. They're the people who "keep it together," who handle crises calmly, who never seem to break down.
But emotional suppression has a cost. The psyche doesn't distinguish between emotions to be suppressed — pushing down sadness also pushes down joy; blocking anxiety also blocks excitement. Over time, emotional suppression creates emotional flatness where nothing feels very much of anything. The person functions but doesn't really live. They perform competence while experiencing anhedonia — the inability to feel pleasure that's a hallmark of depression.
Moreover, suppressed emotions don't disappear — they accumulate. The sadness not felt becomes chronic low-grade depression. The anger not expressed becomes persistent irritability. The grief not processed becomes pervasive emptiness. The person maintains external equilibrium while internal pressure builds, often eventually emerging as physical symptoms, sudden breakdowns, or deepening depression.
The Perfectionism-Depression Connection
Perfectionism and depression are deeply intertwined, each feeding the other in destructive cycles. Perfectionism drives relentless self-criticism that erodes self-worth. It creates impossible standards that guarantee failure and disappointment. It transforms every accomplishment into evidence of inadequacy (focus on what could have been better) rather than genuine achievement.
For high-functioning depressed individuals, perfectionism serves multiple functions. It drives the achievement that maintains identity and external validation. It provides structure and control in a life that feels internally chaotic. It focuses attention outward on tasks and standards rather than inward on painful emotions.
But perfectionism also maintains depression. The harsh inner critic that demands perfection ensures the person never feels good enough. The all-or-nothing thinking that underlies perfectionism means partial success feels like complete failure. The fear of failure that drives perfectionist striving also prevents risk-taking, growth, and the self-compassion needed for recovery.
High-functioning depression often involves what appears externally as impressive competence while internally the person experiences constant self-attack. They achieve at high levels while believing they're frauds about to be exposed. They receive praise while hearing only criticism in their own minds. The external success and internal self-loathing coexist in exhausting contradiction.

Author: Evan Miller;
Source: psychology10.click
Recognizing the Signs: What High-Functioning Depression Actually Looks Like
The Exhaustion That Sleep Doesn't Fix
The fatigue of high-functioning depression differs qualitatively from ordinary tiredness. It's not the tiredness that follows exertion and resolves with rest. It's a bone-deep weariness that persists regardless of sleep, a heaviness that makes everything feel harder than it should be.
People describe waking after eight hours feeling unrested, as if they'd been working all night rather than sleeping. Coffee provides temporary alertness but not genuine energy. By afternoon they're running on fumes, powered by willpower and caffeine rather than actual vitality. Weekends of rest don't restore them — they might sleep more but feel no more rested.
This fatigue reflects depression's impact on brain chemistry, sleep architecture, and energy regulation. Even when sleep duration seems adequate, depression disrupts the restorative stages of sleep. The brain doesn't fully rest even when the body does. Additionally, the constant effort of maintaining functionality while depressed depletes resources faster than rest can replenish.
The exhaustion affects everything but shows nowhere. The person continues meeting responsibilities, perhaps even excelling, but the cost is invisible. They're climbing mountains while appearing to walk on flat ground, and wondering why they're so tired when nothing seems that hard.
Emptiness Beneath the Surface
Perhaps the most defining feature of high-functioning depression is persistent emptiness that coexists with apparently full life. The person does everything they're supposed to do — works, socializes, exercises, maintains relationships — yet feels hollow inside. There's a gap between going through motions and actually experiencing life.
This emptiness differs from boredom or dissatisfaction. It's not that life is uninteresting — it's that the capacity to be interested has diminished. It's not that accomplishments are meaningless — it's that the ability to feel their meaning has faded. The person stands in the midst of their successful life and feels nothing, or feels only the dull ache of knowing they should feel something and can't.
Accomplishments don't satisfy. The promotion comes, the goal is reached, the milestone passes — and the expected happiness doesn't arrive. There's a brief flicker of relief or pleasure, then the emptiness returns, often deeper than before because now there's no future achievement to hope will fix things. The person has arrived at destinations that were supposed to bring fulfillment and found only more emptiness.
Pleasures don't please. Activities that once brought joy now feel mechanical. Hobbies become obligations. Vacations feel exhausting rather than restorative. Social gatherings are endured rather than enjoyed. The person participates in life but doesn't really inhabit it.
The Irritability Everyone Notices but Misunderstands
Depression is commonly associated with sadness, but in high-functioning presentations it often manifests primarily as irritability. Small things trigger disproportionate frustration. Patience evaporates quickly. The person snaps at loved ones over minor issues, then feels guilty without understanding why their fuse is so short.
This irritability reflects depleted emotional resources. When internal energy is consumed by maintaining functionality despite depression, there's nothing left for patience, tolerance, and emotional regulation. Every additional demand — even small ones — feels like too much because there's nothing in reserve.
The irritability creates problems that compound depression. Relationships strain under repeated conflicts. The person feels guilty about their short temper, adding self-criticism to existing depression. Others distance themselves, increasing isolation. Work relationships suffer if irritability leaks into professional contexts.
Often the irritability is attributed to external factors — stress, poor sleep, demanding circumstances — without recognizing it as depression symptom. The person might work on stress management while missing the underlying condition. The irritability continues because its actual cause remains unaddressed.
The Performance of Happiness
People with high-functioning depression become skilled performers of emotions they don't feel. They smile when expected, laugh at appropriate moments, express enthusiasm when required. The performance can be convincing enough to fool everyone, including sometimes themselves.
But there's a qualitative difference between felt and performed emotion. The smile doesn't quite reach the eyes. The laugh ends slightly too quickly. The enthusiasm lacks genuine energy. Close observers might sense something off without being able to identify what. The person themselves might notice that positive experiences feel observed rather than felt — they know they're at a party but don't feel like they're at a party.
This emotional performance is exhausting precisely because it's performance. Genuine emotion happens naturally; performed emotion requires constant monitoring and effort. Every interaction demands attention to appropriate responses. Every social situation involves playing a role rather than simply being present.
The performance also deepens depression by reinforcing disconnection from authentic experience. The person becomes increasingly alienated from their own emotional life, unsure what they actually feel versus what they're performing. The gap between external presentation and internal reality widens until they may feel like they don't know who they really are anymore.
Withdrawal Disguised as Busyness
Social withdrawal is a classic depression symptom, but in high-functioning depression it hides behind legitimate-sounding explanations. The person rarely sees friends, but there's always a valid reason — work deadlines, family obligations, conflicting schedules, exhaustion from the week.
The busyness isn't fabricated — high-functioning depressed people often are genuinely busy, sometimes compulsively so, using work and obligations to avoid the emptiness that emerges in unstructured time. But the busyness also provides socially acceptable cover for withdrawal that might otherwise raise concern.
The withdrawal happens gradually. First one gathering is skipped due to genuine tiredness. Then the next invitation feels like too much. Slowly the social world contracts as the person increasingly chooses isolation over the effort of connection. The few relationships maintained become more superficial as the person lacks energy for genuine intimacy.
Meanwhile, the isolation worsens depression. Humans are social creatures; connection is a psychological need, not just a preference. Withdrawal removes one of the most potent natural antidepressants — genuine human connection — while providing more time alone with depressive thoughts. The person isolates to protect themselves from demands they can't meet, but the isolation accelerates the decline they're trying to manage.
Impact on Close Relationships
High-functioning depression doesn't just affect the person experiencing it — it affects everyone close to them, often in ways neither party fully understands. Partners, family members, and close friends sense something is wrong without being able to identify what. They might experience the person as distant, irritable, emotionally unavailable, or simply not present even when physically there.
The person with high-functioning depression often can't explain what's happening because they don't fully recognize it themselves. They might deflect concerns with reassurances that everything is fine, leaving loved ones confused about whether to trust their own perceptions. The gap between the person's assertions ("I'm fine") and their behavior (withdrawn, empty, irritable) creates confusion and sometimes conflict.
Relationships suffer from the emotional performance that characterizes high-functioning depression. When one partner is constantly performing rather than genuinely present, intimacy erodes. The depressed person may feel increasingly isolated even within relationships, unable to share their actual experience. Their partner may feel shut out, confused, or responsible for a problem they can't identify.
Recognition and treatment of high-functioning depression often improves relationships significantly. When the person can acknowledge what's happening and begin to show up authentically, connection becomes possible again. Partners and family members, understanding the situation, can offer support rather than frustration. The isolation that maintained depression begins to break down.
The Physical Manifestations
Depression doesn't respect the artificial mind-body divide. It manifests physically through multiple pathways, creating symptoms that often get addressed medically without recognizing their psychological origin.
Chronic pain without clear cause — headaches, back pain, muscle tension — can reflect depression's physical expression. The somatization of psychological distress creates genuine physical symptoms, not imagined ones. The person really does hurt; the origin is depression rather than tissue damage.
Digestive issues frequently accompany depression. The gut-brain connection means emotional states directly affect digestive function. The person might chase gastroenterological diagnoses for years without recognizing depression as the underlying factor.
Sleep disturbance — difficulty falling asleep, staying asleep, or waking rested — both results from and contributes to depression. The person might address sleep with medication or behavioral techniques while missing that depression is disrupting sleep architecture.
These physical manifestations often receive medical attention without psychological evaluation. The person accumulates diagnoses — chronic fatigue, fibromyalgia, irritable bowel, tension headaches — while the underlying depression continues unaddressed. Treating symptoms without treating cause provides limited relief.
The Dangerous Self-Deceptions
"I Can't Be Depressed Because..."
High-functioning depression survives through a series of self-deceptions that invalidate the person's own experience. These internal arguments feel logical but serve to deny depression rather than assess it accurately.
"I can't be depressed because I'm still productive." This confuses depression with incapacity. Depression is an internal experience, not a performance metric. Many depressed people remain productive through enormous effort, habit, or fear of consequences. Productivity proves willpower, not wellness.
"I can't be depressed because my life is good." This confuses circumstances with internal states. Depression is a brain-based condition that can occur regardless of external circumstances. Having a good life doesn't immunize against depression any more than it immunizes against diabetes or chronic pain.
"I can't be depressed because I don't feel sad." This reflects a narrow understanding of depression. While sadness can be present, depression also manifests as emptiness, numbness, irritability, exhaustion, and loss of pleasure. The absence of dramatic sadness doesn't indicate absence of depression.
"I can't be depressed because I still enjoy some things." This sets an impossibly high bar for depression. Few depressed people experience complete anhedonia — usually there's diminished rather than absent pleasure. Enjoying some things while finding most of life empty and exhausting is entirely consistent with depression.
These self-deceptions serve short-term psychological protection but prevent the recognition and treatment that would actually help. The person maintains an identity as someone who is fine while becoming progressively less fine.
The Comparison Trap
High-functioning depressed individuals often dismiss their suffering through comparison — to people with "real" depression, to those with harder circumstances, to images of what depression "should" look like.
"Other people have it worse." This is almost always true and completely irrelevant. The existence of greater suffering elsewhere doesn't diminish the reality of present suffering. By this logic, only the single most suffering person in the world would be entitled to acknowledgment or help.
"Real depression means you can't function." This creates a dangerous paradox where only severely impaired depression counts as real, ensuring that millions of people with genuine but less visibly severe depression never seek help. It also ignores that high-functioning depression, left untreated, often progresses to less functional states.
"I should be grateful, not depressed." Gratitude and depression aren't mutually exclusive. A person can genuinely appreciate their circumstances while experiencing a brain-based condition that impairs mood and energy. The pressure to feel grateful for things that depression prevents enjoying adds shame to suffering.
These comparisons serve to invalidate experience and prevent help-seeking. They also reflect the perfectionism common in high-functioning depression — even in acknowledging suffering, there's a sense of not suffering correctly or sufficiently.
When someone comes to me with years of unexplained physical symptoms and a history of inconclusive medical workups, depression is one of the first things I explore. The mind and body aren't separate — psychological suffering manifests physically. Some of my most physically symptomatic patients have been people with unrecognized high-functioning depression. Their bodies were expressing what their minds wouldn't acknowledge.
— Dr. Rachel Kim, Psychiatrist and Author, UCLA Health Depression Program
Why High-Functioning Depression Goes Untreated
The Functionality Paradox
The very functioning that defines this depression type also prevents treatment. The person continues meeting responsibilities, so no external crisis forces confrontation with the problem. They maintain appearances well enough that no one intervenes. They cope effectively enough that they can continue coping, at least for a while.
This creates what might be called the functionality paradox: the better someone manages their depression, the less likely they are to get help for it. Their coping skills become obstacles to recovery because they enable continued functioning without treatment.
The paradox is compounded by healthcare systems that often require significant impairment before providing mental health services. The person might not meet criteria for intensive treatment, might face long waits for therapy, might not be taken seriously when they describe symptoms alongside continued functioning. The system designed to help can inadvertently validate the belief that their suffering doesn't qualify.
Identity Threat
For achievement-oriented individuals, acknowledging depression threatens core identity. They've built self-understanding around competence, capability, and success. Depression feels like failure — not just a condition they have, but evidence of who they fundamentally are.
This identity threat makes seeking help feel like admitting defeat rather than accessing appropriate medical care. The person might readily see a doctor for a physical condition but resist mental health care because of what it implies about them. They might intellectually know depression is a treatable condition while emotionally experiencing it as character flaw.
The stigma around mental health, though decreasing, reinforces identity threat. Concerns about how others would view them, whether it would affect their career, whether they'd be seen as weak or unreliable — these fears prevent help-seeking even when the person recognizes something is wrong.
The "Just Push Through" Mentality
Many high-functioning depressed individuals have succeeded in life precisely through pushing through difficulty. They've developed tremendous capacity for perseverance, for continuing despite obstacles, for not letting internal states derail external performance.
This strength becomes liability when applied to depression. The person approaches depression as another obstacle to push through rather than a condition requiring treatment. They apply more effort, more willpower, more determination — strategies that might work for many challenges but don't work for brain-based conditions.
The push-through mentality is often reinforced by past success. "I've gotten through hard things before. I can get through this." But depression isn't something to get through by effort alone. The very brain systems that would generate effective effort are impaired. Pushing through depletes resources faster than they regenerate, eventually leading to exhaustion that can no longer be overridden.

Author: Evan Miller;
Source: psychology10.click
The Path Forward: Recognition, Treatment, and Recovery
Breaking Through Denial
The first step is often the hardest: acknowledging that despite functioning, despite achievements, despite maintained appearances, something is genuinely wrong. This acknowledgment doesn't mean accepting defeat — it means accepting reality so it can be addressed.
Questions that can break through denial include asking yourself whether you would accept this level of internal suffering in someone you love. Consider whether functioning is the same as thriving. Reflect on what you would tell a friend describing your experience. Ask honestly whether you're surviving or actually living, and consider what maintaining this functioning is costing you.
The goal isn't self-diagnosis but honest self-assessment that can lead to professional evaluation. The person doesn't need to be certain they're depressed — they need to be honest enough about their experience to seek appropriate assessment.
Professional Evaluation and Treatment
High-functioning depression responds to the same treatments as other depression forms: psychotherapy, medication when appropriate, lifestyle interventions, and their combination.
Psychotherapy approaches particularly relevant for high-functioning depression include Cognitive Behavioral Therapy (CBT), which addresses the negative thought patterns and perfectionism that maintain depression. It helps identify and challenge the self-critical thinking, all-or-nothing beliefs, and impossible standards that characterize high-functioning presentations. Psychodynamic therapy explores the underlying patterns — often from childhood — that created the achievement-identity fusion and emotional suppression now maintaining depression. Understanding why functioning became so essential can help release its grip. Acceptance and Commitment Therapy (ACT) helps with accepting difficult internal experiences while committing to values-aligned action. For people who've been fighting or denying their emotional experience, learning acceptance can be transformative.
Medication can help when depression has significant biological components. The decision involves weighing benefits, side effects, and individual factors. Many high-functioning depressed people resist medication, seeing it as admission of inability to cope. Reframing medication as appropriate treatment for a medical condition rather than failure of willpower can help.
Online therapy for depression has made treatment more accessible, removing barriers of scheduling, commuting, and visibility that might prevent high-functioning individuals from seeking help. The convenience and privacy of online options can be particularly appealing to those concerned about being seen entering a therapist's office.
The Recovery Process
Recovery from high-functioning depression often requires more than symptom reduction — it requires restructuring the patterns that created vulnerability to depression in the first place. This is deeper work than simply feeling better; it's becoming someone who doesn't need to maintain exhausting facades to feel worthwhile.
Examining the achievement-identity fusion is often central to recovery. This means building self-worth that doesn't depend entirely on performance, developing sense of inherent value independent of accomplishment, learning that rest and limitation don't equal worthlessness. For many high-functioning depressed individuals, this represents a fundamental shift in how they've understood themselves for decades. The work involves recognizing where achievement-based worth originated, understanding its costs alongside its benefits, and gradually developing alternative sources of self-esteem.
Developing emotional capacity means learning to feel rather than suppress, to express rather than perform, to connect authentically rather than maintaining careful distance. This often feels uncomfortable initially, like exercising muscles that haven't been used in years. Emotions may emerge intensely when suppression finally releases. Therapy provides a safe container for this emotional re-awakening, helping the person tolerate and integrate feelings they've long avoided. Over time, emotional capacity builds — the person becomes able to feel without being overwhelmed, to experience without performing, to connect without exhausting themselves.
Changing relationship with perfectionism involves developing self-compassion, accepting "good enough," tolerating imperfection without self-attack. The inner critic that's driven achievement must be moderated without being entirely silenced. This is delicate work — the goal isn't to eliminate standards but to humanize them, to allow for the imperfection inherent in being human. Self-compassion practices, often incorporated into therapy, help build a kinder internal voice that can coexist with high standards without demanding impossible perfection.
Building sustainable life rather than impressive one means prioritizing wellbeing alongside achievement, creating space for rest and recovery, developing relationships that provide genuine connection rather than just functional interaction. This often requires practical changes — reducing commitments, setting boundaries, protecting time for non-productive activities. For people whose identities have been built on achievement and busyness, these changes can feel threatening at first, like giving up on themselves. In reality, they're making space for genuine living rather than mere performance.
Recovery isn't returning to pre-depression functioning — it's building new patterns more sustainable than those that led to depression. The goal isn't to perform wellness but to actually experience it. This distinction matters: many high-functioning depressed people initially approach recovery the way they approach everything else — as another achievement to accomplish, another performance to perfect. True recovery requires releasing that approach and learning to simply be, imperfectly and authentically, without constant evaluation.
Maintaining Recovery
Recovery from high-functioning depression isn't a destination but an ongoing process. The patterns that created vulnerability — perfectionism, emotional suppression, achievement-based worth — don't disappear entirely. They can reactivate under stress, during transitions, or when old habits seem easier than new ones.
Maintaining recovery involves ongoing attention to warning signs: increasing perfectionism, withdrawal from support systems, return of the performance mindset, neglect of self-care, and the familiar sensation of emptiness creeping back. Early recognition of these signs allows early intervention, preventing full relapse.
It also involves maintaining the practices that support wellbeing: continued therapy (even if less frequent), ongoing self-compassion practice, protected time for genuine rest, nurturing relationships that allow vulnerability. These aren't luxuries to abandon once crisis passes — they're foundations that prevent future crisis.
Many people in recovery find meaning in helping others recognize high-functioning depression. Their experience, once a source of shame, becomes a resource for others struggling to understand their own suffering. The isolation of hidden depression transforms into connection with others who share the experience.
Frequently Asked Questions
Conclusion: You Deserve More Than Functioning
High-functioning depression is real, serious, and treatable. If you've recognized yourself in these descriptions, you're not weak, broken, or fraudulent — you're someone who's been working incredibly hard to hold things together while suffering internally. That effort deserves recognition, and that suffering deserves care.
The fact that you're still functioning isn't evidence against your depression — it's evidence of how hard you've been fighting. But functioning isn't the goal. Surviving isn't the goal. The goal is actually living, not just performing life. The goal is genuine wellbeing, not just impressive productivity.
You don't have to wait until you collapse to deserve help. You don't have to prove your suffering through visible dysfunction. You don't have to earn treatment through failure. The internal experience matters, and if that experience is one of persistent emptiness, exhaustion, and suffering despite external success — that matters. That's treatable. That can change.
Recovery from high-functioning depression is possible. It may require letting go of some functioning temporarily to heal. It may require admitting vulnerability that your identity has been built to hide. It may require redefining success to include wellbeing rather than just achievement. None of this is easy, but all of it is possible.
The first step is simply acknowledging: what you're experiencing is real, it has a name, and help exists. The next step is reaching out for that help — to a therapist, a doctor, a trusted person, or a crisis line. The journey from surviving to thriving begins with one honest acknowledgment that survival alone isn't enough.
You've been strong in hiding your depression. Now be strong in addressing it. The courage to seek help is no less than the courage that's kept you functioning. Use it for healing instead.
Related Stories
Read more

Read more




The content on psychology10.click is provided for general informational and inspirational purposes only. It is intended to share evidence-based insights and perspectives on psychology, relationships, emotions, and human behavior, and should not be considered professional psychological, medical, therapeutic, or counseling advice.
All information, articles, and materials presented on this website are for general educational purposes only. Individual experiences, emotional responses, mental health needs, and relationship dynamics may vary, and outcomes may differ from person to person.
Psychology10.click makes no representations or warranties regarding the accuracy, completeness, or reliability of the content provided and is not responsible for any errors or omissions, or for decisions or actions taken based on the information presented on this website. Readers are encouraged to seek qualified professional support when dealing with personal mental health or relationship concerns.